
Limb amputations can be extremely debilitating, especially
to those who lose an arm above the shoulder. If you think about it, the
majority of tasks you complete each and every day revolve around the use of
your arm and hands. Without this vital limb, most jobs become overly arduous
and some become impossible. This was the case for Les Baugh, who lost both arms
at the shoulder due to an electrical accident when he was younger. Despite his devastating
injury, Baugh might now able to perform daily life tasks thanks to a new prosthetic
arm that is controlled by his thoughts.
In a presentation on Targeted Muscle Reinnervation (TMR),
Dr. Gregory Dumanian explained the use of TMR in creating new prosthetics for
amputee patients. The big problems of previous models of prosthetics for upper limbs
is that those prosthetics can only move one joint at a time and the prosthetic
is controlled by the wrong muscle signals. These prosthetics lack adequate control
methods because the proximal muscles used to generate motions of the prosthetic
hand and wrist are not normally used to direct those movements.

In order to solve that problem, Dumanian integrated TMR into
a new prosthetic limb. Even if an arm is lost, the main nerves in the arm above
the injury are still attached to the brain. What he did not yet know was how to
utilize those signals to create a “smarter” prosthetic. With knowledge that muscle
signals are 100 times stronger than nerve signals, Dumanian was able to create
a technique to both utilize the nerves in the arm and the muscle signal
generated by the innervation of the arm nerves.

With this new procedure and a robotic arm with 26 joints, Mr. Baugh
can use his new Modular Prosthetic Limbs (MLPs) to perform daily tasks that do
not require proximal muscle use. This new technique and prosthetic now allows
for intuitive motion using “smart” signals to generate movement, broadening the
potential for dexterity of prosthetic arms and hands. It also points out the
greater need for “neural-machine interfaces” to provide sensory feedback to a
person with an amputation and allow that person to interact with their environment.
However, there is one issue with the MLP: price of the prosthetic. Currently, the
Johns Hopkins University Applied Physics Lab is in contact with industry
partners to investigate commercial options to make it more affordable for those with upper limb amputations.
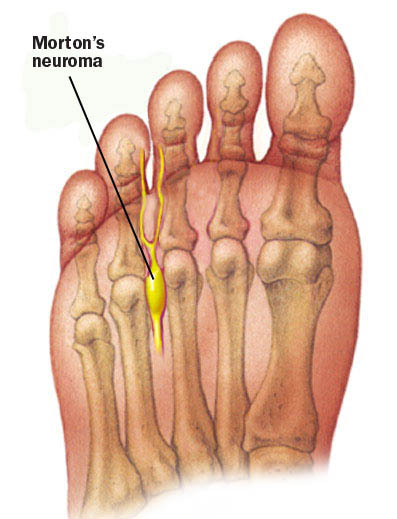 Another interesting feature of Dumanian’s presentation was
the discussion about phantom limb pain. When a sensory nerve is cut, neuromas
are likely to ensue. A neuroma is the swelling of the nerves or growth of the nerve
tissue, which can become very painful. As such, neuromas are very common in patients
with amputations. Dumanian found that when TMR and targeted sensory reinnervation (TSR) were implemented to amputee
patients, their phantom limb pain prevalence decreased. TSR is similar to TMR because the afferent nerves are connected to a different skin surface. After noticing this
correlation, Dumanian began implementing TSR to patients without amputations,
but with painful neuromas. He found significant improvements in pain for those
patients with Morton’s neuromas and neuromas located in other parts of the
body.
Another interesting feature of Dumanian’s presentation was
the discussion about phantom limb pain. When a sensory nerve is cut, neuromas
are likely to ensue. A neuroma is the swelling of the nerves or growth of the nerve
tissue, which can become very painful. As such, neuromas are very common in patients
with amputations. Dumanian found that when TMR and targeted sensory reinnervation (TSR) were implemented to amputee
patients, their phantom limb pain prevalence decreased. TSR is similar to TMR because the afferent nerves are connected to a different skin surface. After noticing this
correlation, Dumanian began implementing TSR to patients without amputations,
but with painful neuromas. He found significant improvements in pain for those
patients with Morton’s neuromas and neuromas located in other parts of the
body.
Sources
Kuiken, Todd A., Laura A. Miller, Robert D. Lipschutz, Blair
A. Lock, Kathy Stubblefield, Paul D. Marasco, Ping Zhou, and Gregory A.
Dumanian. "Targeted Reinnervation for Enhanced Prosthetic Arm Function in
a Woman with a Proximal Amputation: A Case Study." The Lancet
369.9559 (2007): 371-80. Web
No comments:
Post a Comment